Cyclic Vomiting
Overview
CVS was first described in the late 1800s. The key features are
Recurrent discrete episodes of vomiting
Varying intervals of normal (or baseline) health between episodes
Episodes are stereotypical with regard to the timing of onset, symptoms, and duration
The vomiting is not attributable to other disorders
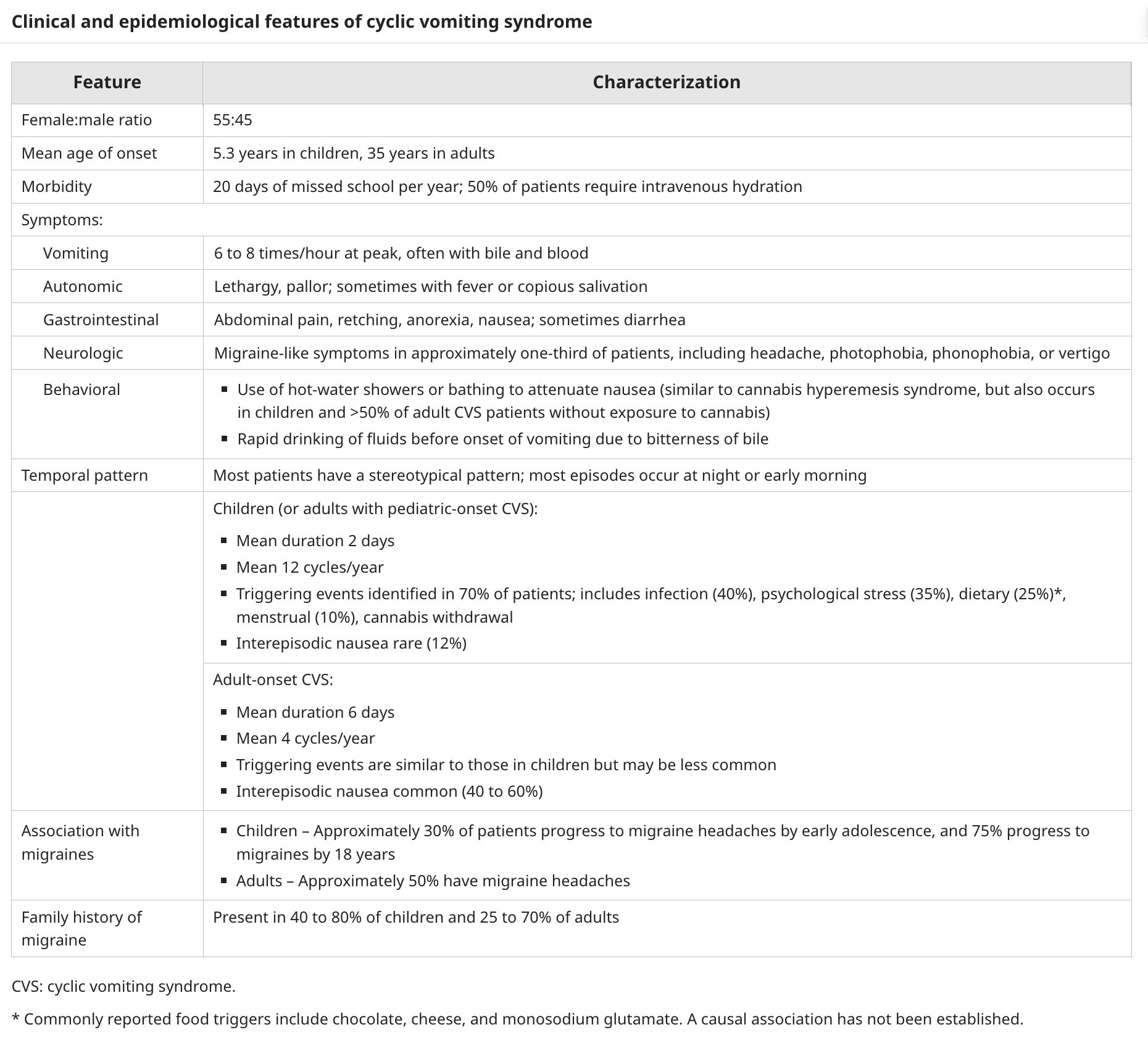
Epidemiology
Prevalence is 2% in children
The average age at diagnosis is 9 years and the average age of symptom onset is 5 years
Prevalence is 1% in adults
Represents 10% of functional gastrointestinal disorders in adults
The average age of symptoms onset in adults is 35 years and diagnosis is 41
Pathogenesis
Unclear
Several potential pathways
Linked to
Autonomic abnormalities with an elevated sympathetic tone
Hypo-pit-adrenal activation
Mitochondrial dysfunction
Oestrogen sensitivity in menses
Food allergy
Cannabis use
One review notes that chronic migraine, epilepsy, panic disorder, and CVS have similar temporal patterns and triggers and posits a neuro-excitability threshold, which when exceeded (due to enhanced susceptibility plus acute stressors), triggers episodic attacks of vomiting
Association with migraine
CVS is linked to migraine headaches and abdominal migraine. In adults, CVS is associated with a personal history (40%) and family history (65%) of migraines and usually responds to antimigraine therapy.
Mitochondrial Dysfunction
Mitochondrial disorders of fatty acid oxidation, respiratory chain defects and mitochondrial deletions can be associated with CVS, usually triggered by infection or prolonged fasting.
Autonomic Dysfunction
Patients with CVS have be found to have augmented sympathetic tone with low parasympathetic tone. Increase association with postural tachycardia, orthostatic hypotension and POTS.
Hypo-Pit-Adrenal
Some kids with CVS have prolonged and severe episodes with profound lethargy, intra-episodic hypertension known as the Sato variant
Oestrogen
Similar to migraines, some girls develop CVS at the onset of their mennstrual periods
Food
Triggers include chocolate, cheese and MSG
Clinical Manifestations
The essential features of CVS are recurring episodes of vomiting with a stereotypical pattern regarding time of onset and duration (hours to days), accompanying symptoms and signs (eg, pallor, lethargy), and the absence of vomiting between episodes
Children
The specific pattern of vomiting episodes is variable but remain typical for each individual patient.
In general, CVS episodes tend to begin in the early morning hours (2:00 to 7:00 AM) and last approximately the same duration. Most have a prodromal period of pallor, anorexia, nausea, abdominal pain, and/or lethargy. The attacks usually last an average of 24 to 48 hours, although they may last up to 7 to 10 days. Approximately one-half of children have attacks at regular intervals, commonly occurring every two to four weeks, while the remainder has unpredictable intervals between episodes. Approximately three-quarters of parents can identify triggers, which are usually psychological (typically more excitement, eg, birthdays, rather than negative stressors) or infectious (eg, upper respiratory) events
Comorbid conditions
Anxiety - 50% of kids with CVS
POTS - 14 to 38%
Adults
Less frequent symptoms than kids
Duration - Longer in adults (6 days versus 2 days)
Triggers - Less common in adults
Behaviours - adults take frequent hot showers and rapidly drink fluids followed by vomiting to dilute the bitterness of the bile
Natural History
Many children outgrow CVS by preteens
Some kids progress from CVS to abdominal migraines and then migraine headaches
Diagnosis
Pediatric criteria — The pediatric criteria for diagnosis of CVS developed by the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition (NASPGHAN) require all of the following:
At least five attacks in any interval or a minimum of three attacks during a six-month period
Episodic attacks of intense nausea and vomiting lasting one hour to 10 days and occurring at least one week apart
Stereotypical pattern and symptoms in the individual patient
Vomiting during attacks occurs at least four times per hour for at least one hour
Return to baseline health between episodes
Not attributed to another disorder
Adult criteria — Criteria for diagnosis of CVS in adults (adult Rome IV criteria) are:
Stereotypical episodes of vomiting regarding onset (acute) and duration (less than one week)
Three or more discrete episodes in the prior year and two episodes in the past six months, occurring at least one week apart
Absence of vomiting between episodes, but other milder symptoms can be present between cycles
Management
Lifestyle interventions to reduce the risk of inducing an attack and improve self-efficacy and quality of life.
Supportive care, provided during any severe bout of cyclic vomiting. This may include admission to the emergency department and/or hospital, intravenous fluids, antiemetics (including those with beneficial sedating effects), and analgesics.
Abortive medication used during the prodrome to prevent or attenuate the attack. This approach may be sufficient for patients with relatively mild or infrequent symptoms and, if possible, should be initiated at home.
Prophylactic medication for selected patients, given daily to prevent further episodes. This approach is generally reserved for patients with frequent prolonged or severe symptoms.
Reference
Cyclic Vomiting Syndrome - UTD
